Ontario’s new FHO+ model marks an important shift in how physicians are compensated, recognizing the time physicians spend across different types of care, not just face-to-face visits.
Beginning April 1, 2026, the model introduces hourly billing for direct care, indirect care, and clinical administration.
While this shift better acknowledges the full scope of your day-to-day work, it also brings new rules, thresholds, and fee codes to navigate. Understanding how FHO+ hourly billing in Ontario works is essential to staying within billing guidelines and maximizing revenue.
What is Changing Under the FHO+ Hourly Billing Model?
At a high level, FHO+ introduces a time-based component to compensation.
Physicians are paid $80 per hour for time spent delivering insured services to rostered patients, including:
- Direct patient care
- Indirect patient care
- Clinical administrative work
This applies across in-basket and out-of-basket services, as well as care provided in long-term care settings and work done after-hours.
FHO+ Hourly Billing Categories and Fee Codes
A key part of working within FHO+ is understanding how your time is categorized. Each category has its own billing code and rules.
Direct Patient Care (Q310 fee code)
This fee code reflects the time spent actively seeing patients.
Direct care is compensated at $80/hour and includes:
- In-person visits
- *Virtual visits (video and telephone)
- Clinical teaching alongside patient care
*Video visits can be performed at or outside the clinic, while telephone care can only be paid at $80/hour at the clinic.
Direct Telephone-Based Care (Q311 fee code)
Telephone care provided outside the clinic is billed separately at $68/hour. Physicians must be present in Ontario to be able to bill Q311, as it is not allowed to bill for services provided while outside of the province.
Indirect Patient Care (Q312 fee code)
Not all patient care happens face-to-face. Indirect care recognizes the work done behind the scenes to support patient outcomes.
Indirect care includes patient-specific tasks such as:
- Charting and documentation
- Reviewing labs, imaging, consult notes
- Care coordination and planning
- Referrals and requisitions
- Patient-related communication (pre/post care)
- Case discussions with other providers and patient-specific clinical teaching are also billed at $80/hour, regardless of location.
It’s also important to note that uninsured services will not be included in this rate.
Clinical Administration (Q313 fee code)
In addition to patient-specific work, physicians spend time on broader activities that support care delivery at a systems level.
Clinical administration covers:
- Preventive care planning
- Chronic disease initiatives
- EMR updates
- Quality improvement work
Non-clinical tasks (e.g., HR, finance, accounting) are not eligible to be billed under clinical administration.
As with indirect care, this is billed at $80/hour and remains the same whether the work is completed in-office or out-of-office.
For all three categories, relativity rates for fiscal year 2026-2027 will apply to hourly payments.
Together, direct care, indirect care, and clinical administration create a more comprehensive framework for recognizing the full scope of physician work under the hourly model.
Hourly Billing Submission Rules
To successfully bill hourly codes, physicians must follow specific submission requirements:
- Health card number, version code, and birthdate fields must be left blank
- Claims submitted with these fields populated will be rejected:
- VHB – No HN required
- VH1 – Invalid Health Number
Additional rules:
- Locums must bill under the FHO group number. Non-FHO physicians cannot bill these codes (EPA rejection)
- Income stabilization physicians are not eligible
Billing Units and Limits Under FHO+
While the hourly model introduces more flexibility, it also comes with clear rules around how time is calculated and capped.
Time Calculation
To ensure consistency, time billing is structured in standardized increments:
- Billed in 15-minute units, calculated cumulatively across the day (1 unit = 15 minutes, 4 units = 60 minutes , etc.)
- For example, Q310, Q312 and Q313 are paid at $20 per unit ($80 per hour)
- Q311 is paid at $17 per unit ($68 per hour)
- 8+ minutes rounds up to a full unit
Maximum Billing Limits
There are daily and rolling limits that physicians must stay within. You can bill up to:
- 14 hours/day (56 units)
- 240 hours per 28-day cycle
Pro-rated monthly limits:
- 28 days → 240 hours (960 units)
- 29 days → 248.6 hours (995 units)
- 30 days → 257.1 hours (1,029 units)
- 31 days → 265.7 hours (1,063 units)
If limits are exceeded:
- Daily → paid at $0 (MD error code)
- Monthly → paid at $0 (M5 error code)
Category Caps
In addition to total hours, there are also limits on how time can be distributed:
- 25% maximum for indirect care + clinical administration combined
- Out of the 25%, 5% maximum for clinical administration out of the combined direct and indirect care hours
This means: For every 3 hours of direct care, you can bill up to an hour of indirect/admin work.
Understanding these ratios is critical to ensuring you are not billing over the maximum while fully capturing eligible time under the model.
The Ministry has stated that any claims billed over the threshold will be returned as errors, and physicians will need to reconcile them and resubmit them, as with most day-to-day claims.
What Is Not Billable Under the FHO+ Hourly Rate?
It’s important to understand that the hourly rate applies specifically to services delivered within the core family practice setting. The hourly model does not apply to:
- Care delivered in emergency departments
- In-hospital services, such as hospitalist work or obstetrical care
- Anesthesia services, surgical assists, and Independent Health Facility (IHF) work
- Services provided to non-rostered or uninsured patients
- Uninsured services, such as prescription refills and form completion
Documentation Requirements for FHO+ Hourly Billing
With a time-based model, maintaining clear, consistent documentation will be essential to ensuring compliance and supporting your billed hours. You are required to maintain records of your total time spent in each category per day.
Physicians must maintain records of:
- Total hours per category
- Brief activity descriptions (for indirect/admin)
Example of documentation summaries:
“April 1 — Indirect Care — 1 hour — chart reviews”
“April 1 — Direct Care — 4 hours”
“April 1 — Direct Telephone Care — 1 hour”
Only the total daily duration needs to be recorded — you are not required to document specific start and stop times. Documentation also does not need to be maintained at the individual patient level.
When submitting codes, it’s a best practice to create a test patient in your EMR (without a date of birth or health card number). Physicians should add a chart entry for each service date when hourly codes are billed to document exactly what the claimed time units include.
It’s also a best practice to submit these codes daily, as you would with your normal day-to-day claims, rather than waiting until the end of the month to bill. The OHIP submission cut-off dates remain applicable to these codes.
As with other insured services, the Ministry may request copies of your records at any time. Maintaining clear, consistent documentation will be essential to ensuring compliance and supporting your billed hours.
Example: Billable vs Worked Hours
To understand how hourly billing limits apply in practice, it helps to look at a real-world scenario. A physician working 97 hours per week may bill only 72 hours, in accordance with the indirect care and CAT limits.
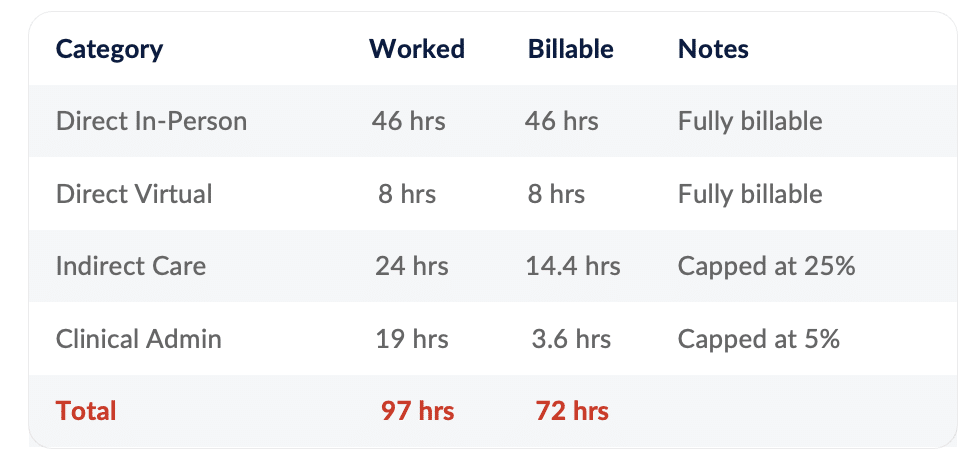
The maximum billable hours for each hourly billing category are for a 28-day period. This means that if you go over in one category one week, you can compensate by working fewer hours in this category another week in the same 28-day period.
In addition to the hourly rate for your work, you are paid shadow billing, capitation and other bonuses, so the hourly rate alone does not reflect your total compensation for work provided.
Tracking these limits is important to avoid unbilled time and better understand where adjustments may be needed
FHO+ Locum and Home Visit Billing
For home visits to your rostered patients, you may bill at the hourly rate for the time spent providing care, as well as for any associated documentation or charting related to that visit. However, travel time is not eligible for billing under the hourly rate.
If you get a locum to cover your FHO practice, the locum is eligible to bill and receive payment under the hourly model when providing services to the FHO’s enrolled patients.
The key requirement is that the locum must be properly registered through the appropriate FHO channels. Ensuring this is completed in advance is important to avoid billing issues or payment delays.
If you’re planning locum coverage, confirming registration and eligibility ahead of time will help ensure a smooth transition and avoid delays.
How DoctorCare Supports Physicians with FHO+ Hourly Billing
With FHO+ now in effect, billing is no longer just about submitting codes. It requires ongoing tracking, monitoring, and adjustments.
DoctorCare supports physicians by helping ensure hourly codes are billed accurately and consistently, reducing the administrative effort required to manage these new requirements. From proper code selection and submission to identifying and correcting issues, our team works to minimize errors and streamline the billing process.
Our goal is to help physicians capture all eligible revenue, stay within billing thresholds, correct rejected claims and reduce administrative burden.
Final Thoughts
The FHO+ hourly billing model better reflects the full scope of physician work, including time spent outside of patient visits. At the same time, it introduces new layers of complexity that require more structured tracking and oversight.
Physicians who actively monitor their billing, time allocation, and documentation will be better positioned to adapt to the FHO+ model and make the most of available billing opportunities.
Need Help Navigating FHO+?
Understanding FHO+ is one thing; optimizing your billing under it is another.
DoctorCare works with physicians to review billing, identify gaps, uncover revenue opportunities, and provide ongoing support under FHO+.
Contact us today to request a complimentary FHO+ income analysis with our team and learn how we can support your practice under FHO+.